

When your patients test negative for acetylcholine receptor (AChR) antibodies,
Look out for Lambert-Eaton myasthenic syndrome (LEMS)1,4
LEMS is a rare neuromuscular disorder with symptoms that overlap those of myasthenia gravis (MG). Take the next step toward diagnostic clarity with a voltage-gated calcium channel (VGCC) antibody test and/or electrodiagnostic test.1,4
Learn more about diagnosing and testing to rule out LEMS.
DIAGNOSTIC CRITERIA AND TESTING
Key LEMS signs and symptoms to watch for during a patient history and initial physical exam4
Start with a patient history
- A history of autoimmune disease is sometimes present in patients with LEMS not associated with cancer4,9,12
Probe for autonomic symptoms
- Dry mouth and impotence are commonly seen in LEMS4
Test the patient’s tendon reflexes
- Hyporeflexia and areflexia are commonly noted in LEMS4
Ask the patient to rise from a chair
- Proximal leg muscle weakness is very common in LEMS4

A diagnosis of LEMS may be suspected based on clinical symptomatology, including proximal muscle weakness, autonomic dysfunction, and hyporeflexia or areflexia. However, confirmatory tests may be helpful in making a definitive diagnosis.4
SYMPTOM TRACKING JOURNAL
Help your patients track their symptoms
MY NEXT STEP is a customizable patient journal that your patients can download and use to keep an accurate record of their symptoms and response to treatment. The details can help inform your diagnostic, treatment, and titration processes while also expediting their return to improved muscle strength and mobility.
Tests that can confirm a diagnosis of LEMS
If clinical examination leads you to suspect LEMS, confirmatory diagnosis may be
made using one or both of the following test methods:

Anti-VGCC antibody testing
A blood test that measures for elevated levels of VGCC antibodies.4

Electrodiagnostic testing
A nerve stimulation test that measures a muscle’s response to
electric pulses 4
Learn more about these 2 tests below.
ANTI-VGCC ANTIBODY TESTING
Sensitivity for LEMS
Elevated serum titers of autoantibodies to VGCC are found in19:
- 85%-90% of LEMS patients without an associated cancer4
- Virtually 100% of LEMS patients with small cell lung cancer20
- Anti-VGCC antibodies are variably present in LEMS patients with other forms of cancer
Clinical significance
A pathogenic role for anti-VGCC antibodies has been established in LEMS in which autoantibodies target VGCC on the presynaptic nerve terminal of the neuromuscular junction and impair neurotransmission of acetylcholine.20,21
Interpreting results
>30 pmol/L* indicates that the patient is positive for LEMS7
- <30 pmol/L is considered to be a negative test result† and a normal titer level; however:
- A negative test result does not rule out a diagnosis of LEMS1
- Electrodiagnostic testing may be performed as additional confirmation1
*30 pmol/L, or 0.03 nmol/L, is the range for VGCC antibody P/Q-type. Reference ranges may vary based on specific laboratories.
†A negative anti-VGCC titer does not exclude LEMS; up to 15% of patients with LEMS have undetectable anti-VGCC antibody levels.4

Free LEMS antibody test available!
Learn MoreELECTRODIAGNOSTIC TESTING
Sensitivity for LEMS
Repetitive Nerve Stimulation studies are often considered the gold standard for the diagnosis of neuromuscular junction disorders, including LEMS, due to their sensitivity for detecting impairments in neuromuscular transmission.6,22
What tests are utilized?
Electrodiagnostic testing typically includes4,23:
- Nerve conduction studies, including repetitive nerve stimulation (RNS)
- Post-exercise facilitation
- Single fiber electromyography (SFEMG)
- SFEMG may be slightly more sensitive than RNS, but it does not distinguish between myasthenia gravis (MG) and LEMS
Hallmarks of LEMS
In LEMS, RNS abnormalities include4:
- Low CMAP amplitudes
- Decrement ≥10% at low frequency RNS (2-5 Hz)
- Increment >100% after maximum voluntary contraction or at high frequency RNS (50 Hz)
Post-exercise facilitation
- Post-exercise facilitation is often performed first to exclude or confirm a potential diagnosis of LEMS, because this test is simple and relatively painless24
- An increase in CMAP amplitude greater than 100% demonstrated immediately after a brief, 10- to 30-second exercise is a classic electrodiagnostic hallmark of LEMS4,25
- Among patients who do not demonstrate the diagnostic incremental value after 10-second exercise, high-frequency RNS is needed24
- Post-exercise facilitation has a sensitivity of 84%-96% and is 100% specific for LEMS4
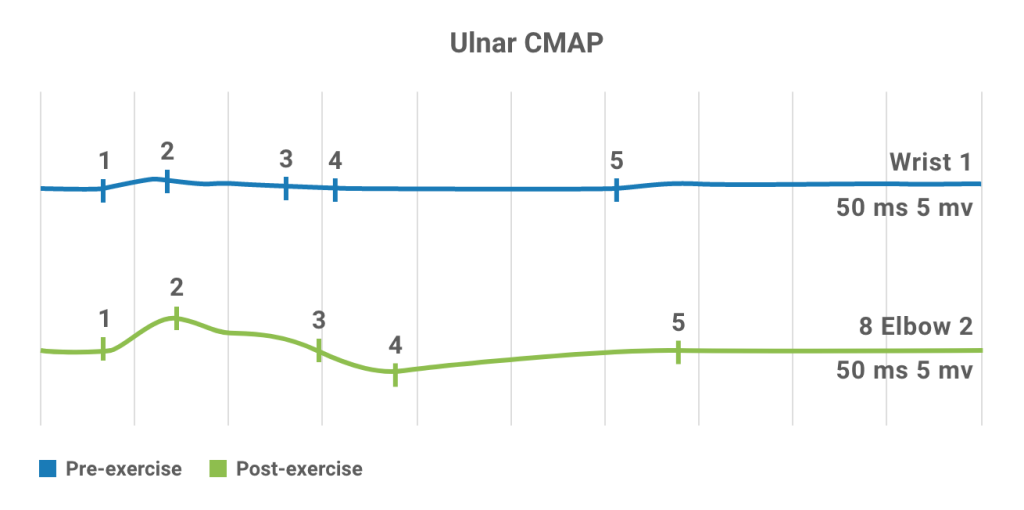
Nerve conduction studies in a patient with LEMS. Baseline CMAP is very small (top).
Following brief exercise, >100% increment is observed in CMAP (bottom), characteristic of LEMS.26
VISUALIZING THE DIAGNOSTIC PROCESS
LEMS diagnosis and oncological screening algorithm27
Start with the Signs & Symptoms tab and then follow the diagnostic process from Signs & Symptoms through Cancer Screening.
SIGNS & SYMPTOMS
Observation of hallmark LEMS signs and symptoms—including proximal muscle weakness, autonomic dysfunction (eg, dry mouth, impotence) and diminished or absent tendon reflexes—should prompt suspicion of LEMS and testing for the presence of anti-VGCC antibodies. Anti-VGCC antibodies are present in virtually all LEMS cases.4

ANTIBODY TESTING
High titers of anti-VGCC antibodies (>30 pmol/L*) indicate a positive diagnosis of LEMS.21 Based on patient history and risk factors, oncologic screening should be considered.4 Evaluate the benefit of treatment of LEMS symptoms with an approved therapy.

Low titers (<30 pmol/L*) suggest a negative or normal diagnosis.21 However, EMG testing should be considered to rule out the possibility of seronegative LEMS. Up to 15% of patients with LEMS have undetectable anti-VGCC antibody levels.4

*30 pmol/L = 0.03nmol/L. Reference ranges may vary based upon specific laboratories.
ELECTRODIAGNOSTIC TESTING (EMG)
Increment on high-frequency nerve stimulation and post-exercise facilitation can provide confirmatory evidence of a diagnosis of LEMS.4 Based on patient history and risk factors, oncologic screening may be considered.27
EMG results consistent with LEMS, together with a negative antibody panel, suggest a diagnosis of seronegative LEMS, or other diagnoses. Based on patient history and risk factors, oncologic screening may be considered.27
Although a clinical diagnosis of LEMS is still possible without a positive EMG result and a negative anti-VGCC antibody panel, the patient is unlikely to have LEMS. Consider investigating another cause for the patient’s symptoms.
CANCER SCREENING
Because up to 60% of LEMS cases are associated with underlying tumor—typically small cell lung cancer (SCLC)—consider screening newly diagnosed LEMS patients for cancer.4,29 Common screening methods may include CT and PET scan, but other test methods may be considered.4
Consult with the oncologist to determine if symptomatic treatment of the patient’s LEMS symptoms would be beneficial.

If no cancer is found, symptomatic treatment should be initiated and follow-up cancer screening should be performed every 6 months for 2 years.

LEMS is a clinically important early indicator of possible cancer; therefore, a LEMS diagnosis should immediately prompt rigorous oncological screening and surveillance.
—Schoser et al, 201727